


If you live with Parkinson’s disease, this is the post I wish I’d read four weeks ago. It might be the most important thing I ever write on this site. Please share it with your caregiver.
Key Takeaways
- Infections in people with Parkinson’s don’t follow the normal rulebook. The first sign is often cognitive — delirium, confusion, sudden personality changes — not pain or fever at the infection site.
- A paronychia (nail infection) almost killed me. Not because the infection itself was severe, but because of how my Parkinson’s-affected brain reacted to it.
- Inflammatory cytokines from the infection cross into a Parkinson’s brain that’s already running on low dopamine and a compromised nervous system. The result is neurological chaos: amplified tremor, lost strength, off-state crashes, dystonia attacks.
- Antibiotics can hit Parkinson’s patients almost as hard as the infection itself — they disrupt levodopa absorption, wipe out gut bacteria, and trigger inflammation in an already vulnerable nervous system.
- Recovery is not days. It’s weeks to months. Post-infection fatigue can last 8 to 16 weeks, sometimes longer.
- If you live alone with Parkinson’s, please read the action steps at the end of this post. What happened to me on my couch could happen to anyone.
“Things Can Always Get Worse” — and This Time They Did
You know what people have reminded me over the years? That things can always get worse. And thank you to everyone who has taken time out of their precious days to pass on that critical information. Things did get worse. How did you know? I never would have guessed.
The last three to four weeks have been the worst experience I’ve endured with Parkinson’s disease since my diagnosis nine years ago. It’s incredible how much a simple fingernail infection — a paronychia — can alter everything about your body. I never imagined a near-death experience could come from one. But it happened. And I need to tell you the full story, because if even one person with Parkinson’s catches an infection earlier because of this post, the last month wasn’t wasted. It was just redirected.
Hi everyone — it’s David from Life With Parkinson’s, and my wife Hayley joins me later in this post to share what this looked like from the caregiver side. If you’re new here, welcome. If you’re returning, thank you. This one’s a heavy read, but it’s important.
What Is a Paronychia, and Why Should People With Parkinson’s Care?
For those who don’t know, a paronychia is a skin infection around a fingernail or toenail. Symptoms include inflammation, swelling, pain, and discomfort. Biting or chewing the nails is a common cause. (I don’t do any of that, and I still don’t know how mine started.) For most people, mild cases can be treated at home. Sounds manageable, right? A finger infection. No big deal.
Wrong.
Here’s the thing I need to hammer into my own brain — and yours, if you have Parkinson’s: infections in people with Parkinson’s do not follow the same symptom list as someone without Parkinson’s. The first sign isn’t always pain or swelling at the infection site. It’s not always something you’d look at and go, “Okay, something is clearly wrong here.” Often, the first sign is in your head, not your finger.
About six months ago, I had a urinary tract infection, and I thought, “Okay, that taught me what I needed to know. A sudden decline in my cognitive abilities means infection.” I had that lesson in my brain. What I didn’t have was a clear picture of what it would actually look like when it happened again — when the infection wasn’t a UTI, but something as mundane as a sore finger.
The Day My Couch Almost Killed Me
If you had to list three places you feel safe in your own home, I bet your couch would make the list. It does for me.
But on this day, my couch nearly ended me.
Here’s what happened. When I’m going off and Hayley needs to run errands, I usually get set up on the couch for a nap. It normally takes 45 minutes, and then I’m back on. But on this day, it took over two hours to reach an on state. Before she left, Hayley made sure I had everything I needed within reach — water, pills, phone, snack. Then she headed out.

About 45 minutes later, my daughter called with a quick question. The moment I sat up to answer, I knew something was wrong. The room began to swirl. I ended the call as fast as I could, took a second round of L-dopa, and tried to lie back down.
I couldn’t.
My body began to panic. My dopamine highway was closing. My body was shutting down. I needed to get horizontal but I was barely holding myself upright. My full-body tremor showed itself. There was nothing I could do except let myself fall back awkwardly into the couch and wait for the meds to kick in.
I tried to call Hayley. The phone was just out of reach, and not set up for voice calls without unlocking it. I could barely move. I was slumped over and struggling to breathe. I knew that if my brain is cut off from meds for more than two hours, or stressed for too long, a dystonia attack happens. After about 30 minutes, I could feel the early signs of one starting.
I also needed to pee. Fifteen minutes later, I peed on the couch.
As I sat there in my own urine, I realized I was not telepathic. Hayley wasn’t getting my mental messages to come home. And I began to feel that I was not going to get out of this alive. I made peace with what was about to happen — a major dystonia attack that would be fatal. Part of those attacks is that my airway constricts, and I usually need Hayley to help open it back up. I knew I was about to suffocate and die from complications related to Parkinson’s. I made my peace with God.
My thumbs bent over as my airway closed — and at exactly that moment, I felt the meds begin to work. Just a glimmer. Just enough. I was able to reach my phone, drag it over without dropping it, and call Hayley, who was actually 90 seconds away.
Thank you, God.
I made my peace with God.
The moment I thought I would die on my own couch.
It took a few hours to recover that day, and I cried a lot. I just could not believe I’d nearly died on my couch alone. I could already see the news headline: “Man killed by couch — safety of living-room furniture to be investigated.“
(One important detail: if we had access to an Inbrija (inhaled levodopa) rescue medication here in Canada — or any equivalent rescue med — this would not have happened. For the love of me, I don’t understand why one isn’t available to us.)
Going Back to the Beginning: The First Clues
About two to three days after my finger first started to hurt, I had a couple of episodes of delirium in the middle of the night. One night I forgot how to fall asleep. The next night I peed the bed and didn’t even wake up. My self-esteem took some pretty big hits.
I want to be very clear about what delirium from an infection looks like when you have Parkinson’s, because I think it’s the single most important thing I can share with you.
It’s not waking up a little foggy. It’s not just confusion. My brain stopped working the way it’s supposed to. I couldn’t tell what was real. I couldn’t communicate. Hayley was watching me, and the person she knows was just gone. Because I have Parkinson’s, the infection amplified every single symptom I already had. My stiffness got worse. My motor function got worse. My ability to think and process — gone. We didn’t know why. I lost all my strength. I was a baby again. At times I couldn’t lift my own hands. They were just too heavy.

Why Infections Hit Parkinson’s Patients So Much Harder
The infection somehow alters your brain chemistry. The research backs this up. When your body fights an infection, it releases inflammatory cytokines — basically little alarm signals your immune system fires off when something is wrong. In a person without Parkinson’s, those signals do their job, your body fights, and you recover.
For us, the brain is already operating with reduced dopamine and a compromised nervous system. Those same inflammatory signals can cross into the brain and cause real neurological chaos. That’s not me being dramatic. That’s the actual mechanism.
Here’s the deeper “why” — the four reasons a simple infection can wreck a person with Parkinson’s:
The brain goes first.
What infection actually looks like in a Parkinson’s body.
1. Cognitive Decline and Delirium Are Often the First Signs
Not a fever. Not pain at the infection site. The brain goes first. For me, with this paronychia, I had a swollen, painful finger — that was real. But what we didn’t connect was that the delirium I was experiencing at night was directly related to the finger. It felt like two completely separate things. It wasn’t.
2. Parkinson’s Can Blunt Your Immune Response
Some research suggests the same neurological changes that affect our movement and cognition also affect how our immune system functions. The normal red flags — “this is serious, fire everything” — may be quieter for us. The usual signals just don’t show up the same way.
3. The Medication Situation Falls Apart
I’ve been on levodopa for nine years. When I’m sick and can’t eat properly, maintaining a precise medication schedule becomes incredibly difficult. When the meds go off schedule, everything else goes off schedule with them. It’s like pulling a card out of a house of cards.
4. Recovery Takes Way Longer
Someone without Parkinson’s might shake off an infection in a week. Are we so lucky? For us, the neurological disruption lingers well after the infection itself is treated. A realistic, evidence-based answer: full recovery from an infection for someone with Parkinson’s can take weeks to several months, even after the infection itself is gone. In some cases, certain symptoms never fully return to pre-infection baseline.
The biggest wild card is post-infection fatigue. In Parkinson’s disease, it can be crushing, persistent, and disproportionate to the infection. It’s triggered by even small amounts of exertion. It’s worse in the afternoon and evening. It can last months — especially after UTIs.
What “Full Recovery” Actually Means for Us
- Motor symptoms return to baseline
- Off periods stabilize
- Cognitive clarity returns
- Energy levels normalize
- No lingering inflammation or immune activation
For many of us, that takes 8 to 16 weeks after the infection is gone. After a UTI, it can take four to six months. For a smaller group, the infection becomes a permanent step down in baseline function. Things can go really sideways.
The Antibiotics Did a Lot of Damage Too
On April 12th in the late afternoon, my finger hurt so badly I knew I needed medical attention. We called our daughter Felicia, and she drove me and Hayley to the hospital. The on-call physician drained my finger — that was the moment we knew it was actually infected. The ride home was when I realized in my heart that there was about to be another problem.
The antibiotics they gave me at the hospital caused major distress. I had a jaw attack on the drive home and barely made it home before my airway closed. I discovered that regular penicillin, even though I needed it, put me into a severe off state. I’d sit on the couch with Hayley and be unable to stop crying. I didn’t have the energy to hold myself up. Hayley described me as “a giant bag of water.” After 3.5 days I had to stop the penicillin entirely. My family doctor switched me to doxycycline for another seven days, which was tolerable but still draining.
Why Antibiotics Hit People With Parkinson’s So Hard
The short version: Parkinson’s changes how your gut, nervous system, and medications interact. Antibiotics hit all three at once. Watch this section with your caregiver — Hayley’s perspective comes next.
- Your gut is already compromised. Parkinson’s affects the enteric nervous system years before motor symptoms. Slower gastric emptying, altered motility, fragile gut lining, less diverse microbiome. Antibiotics wipe out huge sections of gut bacteria in hours. For someone without Parkinson’s that’s a disruption. For someone with it, it’s like pulling out the load-bearing wall of a house.
- Antibiotics interfere with levodopa absorption. When antibiotics kill off the bacteria that help break down food and regulate gut pH, levodopa absorption becomes unpredictable. More off time. More dyskinesia. Sudden fatigue. Feeling washed out.
- Inflammation spikes during antibiotic treatment. Antibiotics don’t just kill bacteria — they trigger an immune response. In Parkinson’s, the nervous system is already more vulnerable to inflammation. Brain fog, worse tremor, mood dips, energy collapse.
- Some antibiotics directly affect the brain. A few classes can cross the blood-brain barrier and cause anxiety, insomnia, dizziness, and worsened tremor. People with Parkinson’s are more sensitive to these effects because dopamine pathways are already stressed.
For someone else, antibiotics are a bump in the road. For me, they’re a system-wide destabilizer.
Hayley’s Perspective: The Caregiver Side
I asked my wife Hayley to share what this experience looked like from her side. Her words, lightly edited for clarity.
“It was really, really hard. I didn’t realize it would be that hard to take care of him afterwards, because he was like a very infant baby. He couldn’t hold up anything — water bottles, pills, anything. He converted into being a baby. That was a lot on me.”
“He was calling me a lot in the night for help. A lot. I didn’t have any time to rest, or charge, or even go pee. I was up again. I think I lost two to three nights of sleep. It’s not worth going to sleep at all when you know you’re just going to go right back in there.”
“With my endometriosis, I wasn’t able to lie down or have a flare-up day. That was hard. Very hard. But I could understand why he couldn’t pick things up. He was floppy — he had no stomach muscles to hold himself up. After I’d do something for him, he’d just flop. And I’d think, where are you going? There’s nowhere else to go.”
“It was scary. I have to say, it was scary. I thought I was going to lose Dave. He looked like he was on death’s door.”
“To other caregivers out there: when you feel frustration coming on, walk out of the room. You can’t get mad. You can’t do anything about it. Just walk out, get some fresh air for a few minutes, and then go back in. Get someone in your family or a friend to sit with them. Just for a little bit. You really do need those few minutes. You really do.”
He looked like he was on death’s door.
Hayley, caregiver and wife.
Hayley balanced caring for me against her own endometriosis flare-ups. She was overworked, exhausted, in pain, and barely sleeping. If you’re a caregiver reading this — please hear her. Walk out of the room. Get help. You need rest too.
A Caregiver Section I Wish We’d Had Before This Happened
If you’re the spouse, partner, adult child, family member, or friend helping someone with Parkinson’s, I want to talk to you directly for a minute.
One of the hardest parts of this infection wasn’t just what it did to me. It was what it did to Hayley. She wasn’t just watching me deal with pain. She was watching my thinking change, my strength disappear, my body stop cooperating, and my personality temporarily slip out of reach. That’s terrifying. And because the infection started in a finger, it didn’t look like something that should be capable of causing that kind of collapse.
That mismatch is what makes Parkinson’s caregiving so difficult. The outside problem can look small while the inside neurological fallout becomes enormous. A caregiver can start out thinking, “This is just a sore finger,” and end the week helping with medications, lifting water bottles, assisting with bathroom accidents, monitoring breathing, watching for delirium, and wondering if their loved one is about to die on the couch.
If that sounds dramatic, I wish it were. It isn’t.
What Caregivers Need to Watch For During an Infection
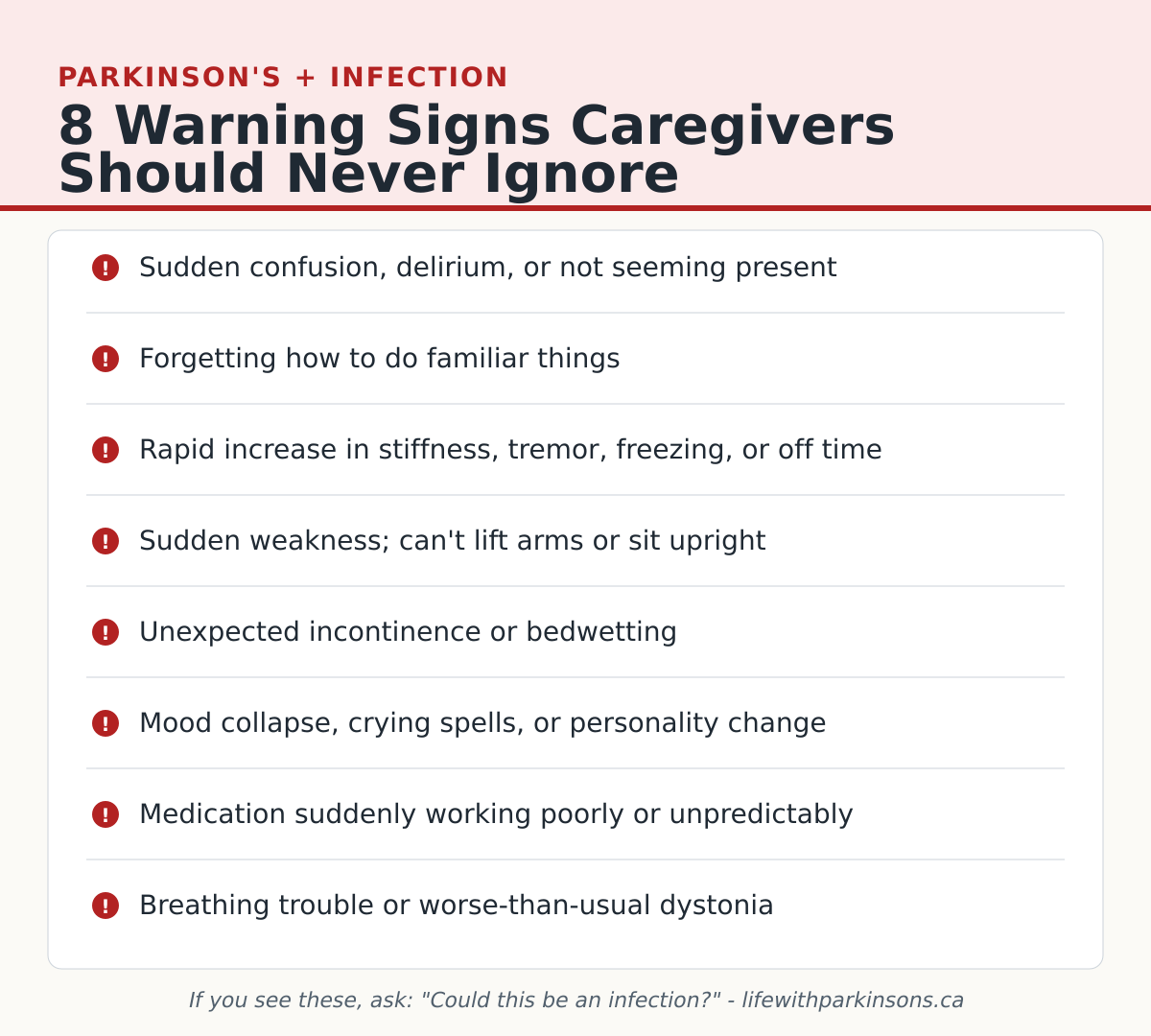
For many people with Parkinson’s, the first sign of infection is not fever. It is not always obvious pain. It is often a sudden change in the brain and body. If you care for someone with Parkinson’s, here are the signs that should make you stop and ask, “Could this be an infection?”
- Sudden confusion, delirium, or not seeming present
- Forgetting how to do familiar things
- Rapid increase in stiffness, tremor, freezing, or off time
- Sudden weakness or inability to lift arms, hold objects, or sit upright
- Unexpected incontinence or bedwetting
- Mood collapse, crying spells, panic, or a dramatic change in personality
- Medication suddenly seeming to work poorly or unpredictably
- Breathing difficulty or dystonia signs that are worse than usual
Those changes are not just “a bad Parkinson’s day.” They may be your only early warning that something serious is brewing.
A Simple Caregiver Action Plan for the Next Time
- Check the body, not just the symptoms. Look for wounds, inflamed nails, urinary symptoms, skin changes, pressure sores, dental pain, fever, or anything else that could point to infection.
- Write down what changed and when. Delirium at 2 a.m., missed medication response, sudden weakness, urinary issues — details matter when you talk to a doctor.
- Do not minimize a small infection. In a Parkinson’s body, “small” and “safe” are not always the same thing.
- Escalate earlier than you think you need to. If cognition changes suddenly, call a doctor, urgent care, or emergency services depending on severity.
- Tell the clinician the Parkinson’s symptoms changed first. That detail matters. Don’t just say, “He has a sore finger.” Say, “He has Parkinson’s, his cognition dropped, his body is shutting down, and he has a finger infection.”
- Watch the antibiotic response closely. If a medication causes a severe off state, airway issues, crying spells, or dramatic worsening, call back and ask about alternatives.
What the Caregiver Needs in a Crisis
This part matters too: the caregiver is not a machine. Hayley was dealing with my crisis while also living with her own pain, exhaustion, and lack of sleep. If you’re in that role, you still need basic human maintenance.
- Keep water and quick food for yourself close by
- Ask a family member or friend to sit with your loved one for even 20–30 minutes
- Step outside and breathe when frustration spikes
- Sleep in shifts if you can; if you can’t, ask for backup the next day
- Write down meds, symptoms, and questions instead of trying to hold everything in your head
- Talk openly about the scary stuff once the crisis passes — don’t carry it alone
Caregiving for Parkinson’s is not just physical labor. It’s emotional load, mental vigilance, and often grief happening in real time. If you need a place to start on that side of things, I’ve written more about communication and respect in caregiving, the mistakes I made accepting help, and stress, anxiety, and role changes.
Caregiver Resources Worth Bookmarking
If you’re supporting someone with Parkinson’s, here are a few reputable places to start. I’m not affiliated with these organizations in a medical sense — I simply want to point people toward credible help.
- Parkinson Canada Resources — A strong Canadian starting point for support groups, webinars, publications, and practical tools.
- Parkinson Canada: Care Partnering — Managing Parkinson’s Together — A practical care-partner guide with self-care tools, communication advice, worksheets, emergency planning, home safety checklists, and support-team planning.
- The Michael J. Fox Foundation: Care Partners and Parkinson’s — Guidance on how care partnership changes over time, emotional realities, communication, and self-care, plus webinars and additional tools.
- Facing Parkinson’s Together: A Guide for Care Partners — A free downloadable guide focused specifically on family caregivers and partners.
- Parkinson’s Foundation — Broad education, helplines, programs, and disease information that can help both the person with Parkinson’s and the caregiver get grounded.
- Davis Phinney Foundation Resources — A wide collection of tools, checklists, and day-to-day living resources for Parkinson’s families.
You do not have to learn all of this the hard way in the middle of a crisis. Bookmark the resources now. Read them when things are calm, not only when everything is on fire.
What You Can Actually Do — Action Steps
I know some of you are reading this and you’re worried. I don’t want to send you away with just the scary stuff. Here’s what to do.
1. Establish the Rule With Your Caregiver: Sudden Cognitive Changes = Medical Emergency
Talk to your partner, family member, or whoever is with you. Make this rule explicit: sudden confusion, delirium, or “not being present” is not just a bad Parkinson’s day. It is a signal that something else may be happening.
Hayley and I have agreed that if I start showing those signs, the very first question she asks is: “Is there any sign of an infection anywhere?” We check, every time, from now on.
2. If You Live Alone, Tell Someone About This
A neighbor, family member, friend — someone who can check in on you regularly. The scary reality is that when delirium hits, you may not be able to advocate for yourself. Set up a system before you need one.
3. Get Wounds and Skin Issues Looked at Early
Don’t wait. With Parkinson’s we normalize discomfort, because we’re already dealing with so much. But a small infection for us is not a small infection. If you have a sore finger, an inflamed nail, a cut that isn’t healing — get it looked at now.
4. Advocate at the ER and Doctor’s Office
If a doctor doesn’t seem to understand why a finger infection caused this level of psychological and neurological disruption — push back. The connection between infection and Parkinson’s symptoms is real, documented, and you deserve a doctor who takes it seriously. Bring your caregiver. Bring this post. Make them listen.
5. Watch for Antibiotic Reactions
If your antibiotic is making your Parkinson’s symptoms dramatically worse — call your doctor. There are alternatives. I had to switch from penicillin to doxycycline, and that switch was the difference between misery and tolerability.
Where I Am Now
The last three to four weeks have felt like a bad horror movie. I’m still not back to where I was before all of this started. But I’m getting there.
If sharing this experience means even one of you catches an infection earlier, or one caregiver recognizes the signs a little quicker — then this month wasn’t wasted. It was just redirected.
An infection should be taken seriously. They can do a lot of harm and linger long after they’ve cleared up. I firmly believe every one of you is doing the best you can with the circumstances you’re in. I hope you never forget that.

Related Reading
- Urinary Tract Infections and Parkinson’s Disease: What You Need to Know Right Now
- What is Parkinson’s Disease? A Comprehensive Guide
- Caregiving 101: Resources & Support for Parkinson’s Care Partners
Help Keep Life With Parkinson’s Going
This site and the YouTube channel run on lived experience and a lot of love. If posts like this one help you or someone you care for, here are two ways to keep the work going – both are completely optional and either one means a lot.
Subscribe to the Newsletter
I send occasional notes – new posts, lessons, and things I wish I’d known sooner. No spam. Easy to unsubscribe.
Become a Channel Member
Channel members support the videos directly on YouTube and get a few perks along the way. If you watch the channel and want to chip in, this is the easiest way.
If this post was helpful, please share it with someone who lives with Parkinson’s or cares for someone who does. We’re building lifewithparkinsons.ca into a lived-experience Parkinson’s resource — and stories like this one are why. Thank you for taking this journey with us.


